General medicine case -8
This is an online e-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs
Chief complaint:-
27 year old male patient came to opd with chief complaints of vomitings ,pedal edema and sob 2 years back.
History of present illness:-
Patient was apparently asymptomatic 2years back then he developed vomitings on 23rd december 2019 which was yellow colored, and non bilious ,non blood stained .He complained of vomiting after taking food and water. After 15 days of onset of vomitings he went to a hospital in suryapet and there for the first time he was diagnosed with BP 170mmHg .He used antihypertensives for 10 days and he stopped after 10 days .
In the month of February again he had 2 -3 episodes of vomitings , decreased urine output ,sob on walking for longer distance .So he visited a hospital in Khammam,all tests were done and there he was diagnosed with renal failure.He was referred to NIMS .There his sob was increased from grade 2 to grade 4 and immediately dialysis was started in NIMS .6 dialysis were done at NIMS.
In the month of March 2020 ,he came to KIMS for dialysis .Since then he is on dialysis weekly twice and continuing antihypertensive drugs (nicardia 20 mg BD)

Past History:-
No history of loose stools , Diabetes Mellitus ,asthama,tuberculosis,epilepsy.
Personal History:-
Diet -mixed
Apetite-Normal
Bowel and bladder movements-regular
Sleep -adequate
No addictions
Family history:- No relevant family history
General examination:-
Patient is conscious,coherent , cooperative and well oriented to time .
Pallor -present



no icterus ,no cyanosis,no lymphadenopathy.

Vitals:-
Temperature-afebrile 98F
Pulse rate -84beats/min
Respiratory rate-16cycles / min
Blood pressure-160/100mmHg
Spo2 at room air-92%
SYSTEMIC EXAMINATION:-
Inspection-chest wall is bilaterally symmetrical.
No precordial bulge .
No engorged veins , visible pulsations ,scars ,sinuses .
Palpation -JVP is normal
Auscultation-S1 S2 heard
RESPIRATORY SYSTEM:-
Position of trachea is central
-Bilateral air entry is normal
Normal vesicular breath sounds were heard
Per abdomen:-
ABDOMEN is nontender
Bowel and bladder sounds heard
No palpable mass or free fluid present

Central Nervous system:-
Patient is conscious
Speech is present
Reflexes are normal
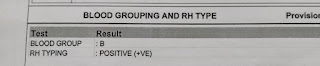
INVESTIGATIONS:-
CUE:-







DIAGNOSIS:-
CKD on MHD with hypertension
Treatment:-


Comments
Post a Comment