General medicine case -6
A 55 year old male who is daily wage worker by occupation came to the OPD complaining about
- Shortness of breath ,pedal edema since 3 months
- cough since 2 months
HISTORY OF PRESENT ILLNESS:
Normal routine of the patient:
He used to get up at 5:00 am in the morning, used to have tea and the time until afternoon talking to his friends then used to have lunch at 1 PM which is rice.He used to return home by 6 in the evening then he used to freshen up and drink alcohol (150-200ml per day) and used to have dinner at 9 PM and sleep after that.
The Patient was apparently asymptomatic 3 months back then he developed bilateral pedal edema which was pitting type , insidious in onset along with swelling of hands and facial puffiness.He also developed sob which was insidious onset , aggravated on doing his work .He also complained of back pain
He also complained of cough since 2 months which was productive .
PAST HISTORY:-
He was chronic alcoholic and smoker since 30 years and stopped alcohol and smoking 2months back .
No history of diabetes Mellitus , hypertension, tuberculosis,asthama .
He had a history of traumatic injury to his right eye while cutting granite stone
The patient is not a known case of diabetes, epilepsy, tuberculosis, asthma, hypertension
Personal history :
- The patient has no loss of appetite
- He takes mixed diet
- No sleep disturbances
- He consumes 90 ml of alcohol daily, was a cigarette smoker 3 months back where he used to take 1pack per day
Family history :
- There are no similar complaints in the family members
Treatment history :
- He is not a known case of drug allergy.
General examination :
Patient is conscious,coherent , cooperative well oriented to time.
Pallor is present (Hb-8.9 /dl)
Icterus -present
No cyanosis
No clubbing of fingers and to
- No lymphadenopathy
- No pedal edema
Vitals :-
Temperature-afebrile
Respiratory rate-20 cycles /min
Pulse rate-72bpm
Blood pressure-140/70mmHg
Spo2-99%at room air
Systemic examination :
CVS-
Inspection - chest wall is bilaterally symmetrical
- No precordial bulge
- No visible pulsations, engorged veins, scars, sinuses
Palpation - JVP is normal
Auscultation - S1 and S2 heard
RESPIRATORY SYSTEM
- Position of trachea is central
- Bilateral air entry is normal
- Normal vesicular breath sounds heard
- No added sounds
PER ABDOMEN
- abdomen is not tender
- bowel and bladder sounds heard
- no palpable mass
- patient has mild amount of fluid
CNS:-
- Patient is conscious
- Speech is present
- Reflexes are norm
Investigations:-







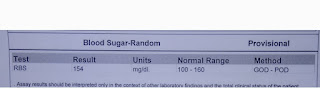
Clinical images:-



TAB. NICARDIA 20 mg BD
2. TAB. NODOSIS 500 mg BD
3. TAB. OROFER XT PO BD
4. INJ. ERYTHROPOIETIN 4000IU WEEKLY ONCE
5. TAB. SHELCAL PO OD
6. INJ. THIAMINE 100 mg in 50 ml NS IV/TID
7. Fluid and Salt restriction


Comments
Post a Comment